 Read article HERE
Read article HERE
Recent Comments
Jeff on Dr.Teel presents to Aging In P… Kim on Elders and Belly Dancing Clara Wentworth on Elders and Belly Dancing
Read Patty Seybold’s blog

Outside Innovation on technology for seniors.- and how Full Circle America is helping her help her mother stay home.
Click HERE to read
Portland Press Herald article about faster internet speeds for Maine talks about Dr.Teel’s Full Circle America program helping more elders.
……”Dr. Chip Teel of Damariscotta uses telemedicine over broadband connections, along with home visits and transportation help, to care for elderly patients at home at a cost of $5,000 per year, as compared to $90,000 per year for a bed at a nursing home.”….Click HERE to read


Scott Donnelly
Nancy Wilder, right, helps Queensbury resident Marylin Pagliuco get into Wilder’s car Thursday, May 30, 2013, for a ride back from a doctor’s appointment in Glens Falls. Wilder has been a member of Aging in Place Glens Falls for about four years, after joining with her ailing mother. She decided to remain with the group after her mother’s death because she knows the day is coming when she will need the services provided by the network. SCOTT DONNELLY–sdonnelly@poststar.com
The meaning of, “There’s no place like home,” evolves as we age.
For a fortunate majority, it will always have its traditional meaning: I’m never more happy than when I’m home. For others, it gets to: There aren’t any elder care options as nice as my home. It can progress to: The challenges of aging are making it so my home isn’t the place I need it to be.
And for a few, it ends up at: There will never again be a place where I feel like I’m home.
Fortunately, the way we care for our aging neighbors is also evolving. It has never been easier for area residents to “age in place,” as the movement is called today. But it’s still not as easy as it’s going to be, if recent efforts gain traction.
“I think aging in place, as a concept, means a lot of different things to a lot of different people,” said Andrew Cruikshank, CEO of Fort Hudson Health System. “We’re all aging in place; we truly are. We’re accessing the services that we need over the course of time.”
Fort Hudson Health System, located in Fort Edward, provides a range of elder care, including both a skilled-care facility and an independent senior housing facility on its campus. It also provides programs for people in the community who need services but aren’t facing so many challenges they need to leave their homes.
Cruikshank said most people are finding alternatives to nursing homes, as new options are developed to help them meet the challenges of old age.
“While there’s a great deal of attention paid to nursing home care as a long-term care provider setting, the reality is the vast majority of long-term care is delivered at home by family and friends,” Cruikshank said. “Nursing home care for the population is actually a smaller percentage.”
The options
Fort Hudson Health System, like most elder care organizations, has evolved significantly over the last decade, Cruikshank said.
“Nursing homes generally aren’t the places they used to be,” he said. “It used to be where an elderly person would come and kind of carry their own suitcases in and say, ‘OK, I’m here, and I’m going to stay here the rest of my life.’ ”
Today, nursing homes are places where many stay just long enough to recover from an illness or medical procedure. They’re places for rehabilitation, with a goal of getting people back into their pre-care lives.
“The vast majority of individuals who are admitted to Fort Hudson return home within 45 days,” Cruikshank said. “Probably 65 to 70 percent of our admissions are coming in with the intention of going home.”
Fort Hudson today has a staff of experts whose job it is to match people with services that can help them return home.
“I would say out of every call that comes into our organization from the community — that comes in on the assumption that Mom or Dad or Grandma or Grandpa now needs nursing home care — the majority of them really don’t, and we’re able to turn them back around and put them in touch with the right resources … to keep them at home longer, if that’s their wish,” Cruikshank said.
Such a plan could include providing in-home care, setting up access to day services or offering information on a number of programs available through other community organizations. Many have their own costs, but those costs rarely rival the price of extended nursing home care.
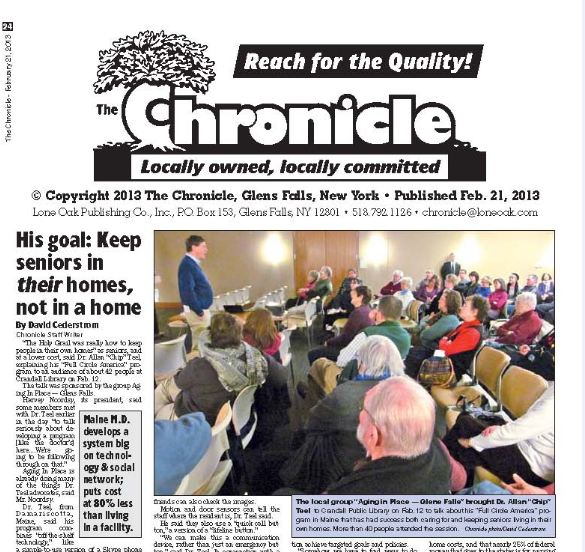
Aging in Place Glens Falls, a grass-roots group started in 2007 by Harvey Noordsy and other Glens Falls area residents, is an example of how things are changing. Noordsy, who is president of the nonprofit agency’s board of directors, was inspired to launch Aging in Place Glens Falls after a brief stay in a retirement community. He and his wife felt they were too young for that kind of housing, so they started doing research.
Noordsy learned about the Village to Village network, a program started in the Boston area that has grown nationwide.
Working off that idea, Aging in Place Glens Falls has a time-bank system, by which volunteers offer their services to others and, in turn, call on the network when they are in need of services. Noordsy said the organization has grown from 15 to 65 members and is providing about 100 hours of volunteer service each month to elderly people in the region.
The cost to join is $20 per year, just enough to cover expenses related to website maintenance and the occasional pamphlet for members, Noordsy said.
The idea is catching on, and there are now five “neighborhood groups,” with another in Lake Luzerne weighing whether to join the network, Noordsy said.
Now, Aging in Place Glens Falls is looking at teaming up with a group called Full Circle America, which builds on the social connections started by the Glens Falls group but adds “virtual assisted living,” which uses technology to help people age in place more safely.
Better aging through technology
Dr. Paul Bachman is a fan of the idea. He has been providing health care in the Adirondacks through Hudson Headwaters Health Network for 27 years, and he thinks new solutions are needed.
“Most of my practice has been a geriatric practice, so I’ve been seeing what everybody knows is coming down the pike — that the elderly population is the most rapidly growing population in our country, and that it won’t be very long before more than 10 or 15 percent of our population is older than 85.”
Specifically, Bachman is seeing a growing number of women living alone in their homes, as they outlive their husbands and their children grow up and leave the area.
“It’s becoming kind of a typical scenario, not only in the country, but certainly in the Adirondacks,” Bachman said.
Through Hudson Headwaters Health Network, and in conjunction with Aging in Place Glens Falls and other regional health care providers, Bachman is hoping to set up a pilot program with Full Circle America by enrolling a few local residents.
The heart of the effort is already in place: a network of community volunteers and health care experts dedicated to providing social support and in-person services ranging from meal preparation to transportation. But what Bachman is hoping to add is a host of in-home technologies that allow the network to be more responsive to members’ needs.
“The Full Circle America concept is taking aging in place to the next level, I think,” Bachman said. “It’s really organizing social support around individual people. It’s also using technology that’s never really been tried in the home before.”
That technology includes sensors on refrigerator and exterior doors of the home, web-based video cameras placed in living areas and one-touch video telephone systems to make it easy for network members to connect with loved ones or other network members. It’s all aimed at making it easy to tell if a person is going about his or her daily routine safely, Bachman said.
“For this to work, you have to have Internet access and broadband, but there are very few places now that don’t have that, to some degree,” he said. “And the Full Circle America program has several levels of subscription.”
Those subscriptions vary based on the amount of technology needed to keep a person safe, but they range from about $350 to about $1,000 per month, Bachman said.
“If a person goes into a nursing home, they could be looking at $100,000 a year,” he said. “So it would be less than 10 percent of the cost of being in a nursing home for the average person participating, and depending on what level of subscription they sign up for, they can have anything from a person who’s checking in on them by telephone and visiting a couple of times a week to full-scale electronic surveillance.”
With services for aging residents also provided through the region’s senior centers, county offices for the aging and organizations such as United Way and the Retired and Senior Volunteer Program, there has never been a better infrastructure in place for aging.
Finding a balance
None of the experts interviewed for this story felt aging in place was, or should be, the goal for all older Americans.
There are those for whom the cost of providing in-home care are prohibitive. Most people who need help with multiple aspects of daily living while also facing chronic health problems can be cared for more efficiently in a skilled nursing facility. And many are likely to benefit more from the social interactions in a good nursing home than they would from sitting in front of a TV in their own living rooms.
“One of the worst culprits of premature demise is the loss of personal touch,” Cruikshank said. “You can keep an individual safe and feed them and hydrate them through a computer, but that is not necessarily going to be healthy. We see seniors all the time saying, ‘I don’t want to go home to my house; there’s no one there. I don’t want to be waiting for my son or daughter to come visit every Tuesday night for an hour.’”
For others, their homes
are located in remote areas too far removed from support infrastructure to make services viable.
Tough lessons
Lynne Michaels of Lake George didn’t realize how hard it would be to help her parents stay in the home they’ve shared for 57 years in Columbia County, an hour-and-a-half drive from Lake George. An early hurdle was convincing her parents to let Lynne and her brothers build a new, one-level home on the property to help them get around in their advancing years, she said.
“We never brought up a nursing home,” Michaels said. “We looked at assisted living, but at that point, it wouldn’t have helped.”
Both of Lynne’s parents had developed cognitive disorders — her mother now has Alzheimer’s disease and her father has dementia. But they also had long-term care insurance, and Michaels decided the resources were there to provide around-the-clock care for them in their home.
Her parents’ insurance policy provided an allowance for in-home care, and she and her siblings are also helping out.
Since those early decisions, though, Michaels found she had to set up a business to manage her parents’ estate and handle payroll, workers’ compensation, taxes and other clerical work related to hiring the five home health aides needed to provide 24/7 care. She said managing the operation has become a part-time job that has given her experiences she hopes others can learn from.
Foremost, she hopes people will have conversations about long-term care with their loved ones. Michaels said she’s already planning for her own long-term care, and has let her children know what she wants. It’s a conversation she never had with her own parents.
“I said this to my children, ‘I wouldn’t want you to
have to take care of me. I would want to go into a nursing facility.’ ”
She also said people should explore their options when it comes time to choose in-home care. She found a lot of the help she needed through a website, Care.com, which provided vetted candidates, Michaels said.
“I’ve been so fortunate to find a young girl who just loves my parents,” she said. That person now lives in her parents’ home, and four other caregivers fill in when the primary caregiver is off.
Aging in place’s future
As the nation’s population ages, health care providers are trying to adapt to the needs of the elderly. But questions about what solutions are coming from the government also have to be considered. Bachman said he hopes the Full Circle America program can be adopted as a national model of elder care. And Cruikshank sees changes coming soon in the way elder care is paid for, especially when it comes to Medicaid.
“New York is shifting to a managed Medicaid environment,” he said. “So, if you require Medicaid-eligible services in the community for a certain period of time — and this is already rolling out downstate — you’re going to be mandatorily enrolled into managed Medicaid long-term care plans.”
As a result, over the next two years, the system will begin to incorporate third-party managed-care payers who will determine what services are necessary for an individual’s care.
“So, they have a vested interest, now, in keeping people in the most cost-effective setting, which many times will be at home getting this care and services,” Cruikshank said. “That will absolutely change the face of how care’s delivered and who’s making determinations as to where it should be delivered.”
We just finished our new Full Circle America video. Click HERE to watch to watch.
to watch.
In September I did another holiday-cum-healthcare-research road trip, this time to those northeastern US states referred to as New England: Massachusetts, Rhode Island, New Hampshire, Maine, Vermont. I was privileged to visit and meet with the leaders of two programs there designed to keep frail elderly people at home, out of nursing homes, and out of the hospital: Dr. Chip Teel of Full Circle America on the coast of Maine ( http://www.fullcircleamerica.com/ ), and Dr. Dennis McCullough, founder of Slow Medicine at Dartmouth University in New Hampshire (details to come in my next post). I felt more than ever that we are on the right track in Vancouver after talking to both of these brilliant innovative guys.
Chip Teel comes across as a high-octane entrepreneur and elder-care visionary. Our first day there, Robin and I had dinner with Chip and his wife Carol at a down-to-earth local pub off the main street of charming Damariscotta, the small Maine town where they live and he practices. The next morning Chip and I sat in his office and discussed his program, he presenting me with a copy of his book Alone and Invisible No More and showing me the system he has in place and hopes to introduce elsewhere, and I peppering him with as many variably relevant questions as I could get in edgewise.
Here’s what I found. Dr. Teel’s vision for home care for frail elderly is based in widely-experienced and genuinely-felt common sense. I was delighted that we agree on many things, confirming my impression from visiting a program in Manhattan in 2010 that our problems and some potential solutions span national borders and health-care systems. The first question Chip asks a new frail elderly patient is, “How do you want to live the rest of your life?” The second, “What can you and your family do for other people in the community?” These open the doors on two fundamentals of his practice: every elderly person is entitled to decide for themselves, and things work best when people help people. He believes in “the dignity of risk”, which means that when you take away someone’s right to live at risk (closely connected to their right to living their lives the way they want to) you dehumanize them, treat them like a commodity, and un-dignify them.
(I can’t avoid mentioning the linguistic entropy that seems relentlessly to destroy constructs like “dignity”, “living at risk”, and also “evidence”, “patient-centeredness”, and now most recently “primary care”. I find the consequence of creating meaninglessness where previously there were critically important ideas terrifying. I’ll try to do a post on this…).
My next lesson from Chip Teel was economic. An American down to his sneakers, he understands the significance of money in health care the way I’m afraid few Canadians do. My own brief foray into the economic impossibility of high-quality interdisciplinary home care of frailty involved a proposal I made to a private-enterprise organization here in Vancouver which was eventually rejected because the dollar numbers didn’t add up. The truth is without new money you have to somehow save money to make frailty-at-home care sensible. Dr. Teel’s answers: first, involve the community. Volunteers in other words. Second, use smart technology.
His presentations, book, and other information about the Full Circle America contain all sorts of examples of next-door neighbors, similar-interest new friends, family members, and kindly souls pitching in to do (usually for free) things that without their help would cost money. Transportation to and from appointments, getting an elderly lady to a nursing home to do a piano concert, teenagers popping in at noon to make sure the old guy up the street has had his breakfast, sort of thing. I’ve heard the criticism from, say, Canada Health Act fundamentalists that a program which relies on volunteers isn’t sustainable or politically correct. And more credibly for me I also hear the one summarized in the comment, “Spoken like someone from a small town.” It’s much harder to develop the kind of networks that work in Damariscotta (pop. just over 2000) than in most neighborhoods in Vancouver with its million and a half people, let alone Toronto or Los Angeles. But that doesn’t mean it can’t be done in some attenuated or different way. The biggest city in the world is made up of an awful lot of neighborhoods. But it takes a sincere intimate experience of each of those neighborhoods to get mutual responsibility going.
Full Circle America will I imagine also be seen by some people (it was initially by me) as a techno-gizmo for sale. It’s far, far, more than that, but there are techno-gizmos involved in its second money-saving idea. Teel monitors his patients with digital cameras, images relayed to a central facility where a technician evaluates images one, two, or more times per day, and automated algorithms trigger warning messages in the event of alarm-features. Opening the exterior door after midnight in winter, out of bed at night for more than 30 minutes, or in the bathroom any time for more than 90 minutes, for example. The inevitable privacy-invasion objection Chip counters by comparison to the much nastier privacy invasions in institutions. Most people would choose little cameras potentially watching their bedroom all night at home over two or three hospital ward door- or curtain-openings without warning by staff with flashlights. By using this monitoring (and the technology gets more sophisticated all the time) people who would otherwise need a 24-hour paid person at home might manage with two 2-hour visits per day and round-the-clock computer surveillance.
Full Circle America isn’t perfect (what is?). I don’t quite share Dr. Teel’s belief in full generalizability of what he’s doing. I think the concepts of micro-cultural cooperation and the use of surveillance technology are portable, but dazzlingly comprehensive attention to detail, one of the program’s great strengths, might be reflected in a certain inflexibility as Chip struggles to reproduce it in other communities. It is at very least an important chunk of what we will eventually use to establish home care of frailty the way everybody knowledgeable knows it needs to be done.
Dr. Teel has confronted the problem many of us know so well, come up with original ideas (some of which have also independently occurred to others), and most critically made them work on the ground where he lives and works. Visionaries like him make the rest of us proud. Spreading the word, pulling networks together, and trying to be as practical as he’s been will I believe help us get where we want to go.
Neighbors Helping Neighbors, that’s what it’s all about. Read HERE
 Photos by George Rizer for the Boston Globe
Photos by George Rizer for the Boston Globe

Discussion on Aging at Home on MPBN
Click <HERE> to watch

Dr. Teel was invited to speak at the Korea Healthcare Congress in Seoul, Korea. He will be introducing Full Circle America’s “Maine Approach” to elder care in two different presentations this week. 행운과 안전 여행
| Jeff on Dr.Teel presents to Aging In P… | |
| Kim on Elders and Belly Dancing | |
| Clara Wentworth on Elders and Belly Dancing |
